Hand Pain
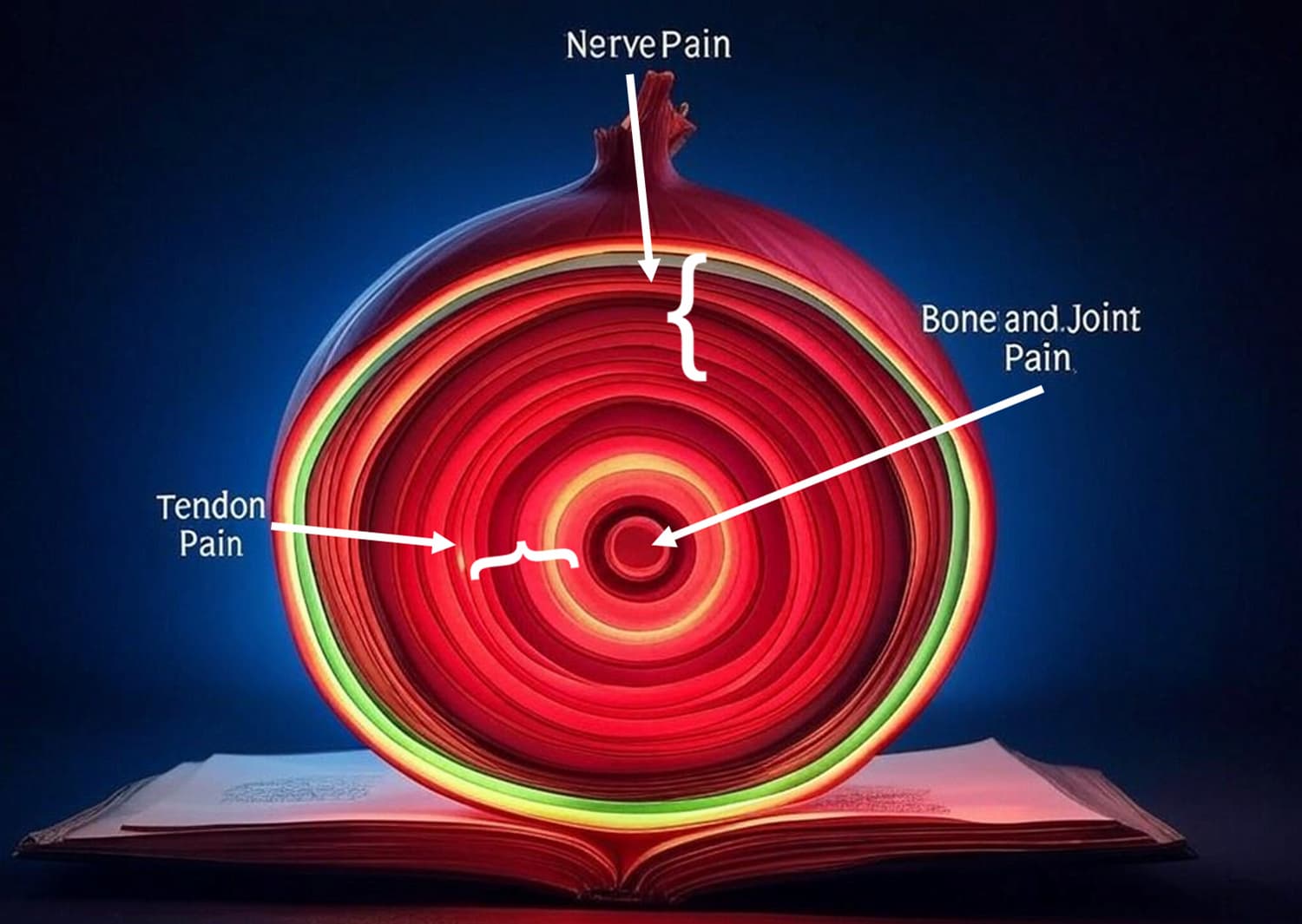
When a patient comes to see me about a hand problem, more often than not it is because of pain. I look at pain like the layers of an onion. Although you may have an x-ray that demonstrates advanced arthritis, the commonest cause for most of the hand pain is nerve dysfunction, such as carpal tunnel syndrome. Slightly less common are the tendon issues such as trigger finger or De Quervain’s in the wrist. Only when these have both been accounted for should we be discussing bone surgery, which is effective only when the other issues have been treated and on its own may not be that bad.
Once the nerve and tendon pain is treated, very often patients no longer feel the need for bone surgery. Nerve and tendon surgery have a faster recovery and are offered in the office setting without the need for a general, or together with the bone and joint surgery.
Location of your surgery is often your choice
Below I have listed things that I offer in the office versus the main operating room. You may always choose to have your simpler procedure in the main operating room, the choice is yours.
Hand procedures offered in the office
- Carpal tunnel release both open and via ultrasound (Sonex)
- Cubital tunnel release
- Gyon’s canal release
- Radial tunnel release
- Lacertus release
- Fat injections to hand joints and tissue
- Trigger finger release
- Hand tumors and ganglions removal
- Mucous cyst removal
- Nail deformity correction
- Dupuytren’s release surgery
- Tenolysis
- Basic hand trauma management including
- K wires for hand fractures
- Nail bed repair
- Tendon repair
- Mallet finger repair
Hand surgery offered in the main operating room
- Hand joint replacement
- Basal Joint arthroplasty
- Wrist arthritis surgery including carpectomy, partial or total wrist fusions
- Finger fusions
- Triangular fibrocartilage repair
- Wrist arthroscopy
- Ulnar shortening
- Carpal bone revascularization
- Kienbock’s disease and scaphoid non-union
- Scaphoid fracture management
- Wrist fracture management
Plastic Surgical procedures
I am a broadly trained Plastic Surgeon, offering skin cancer reconstruction and body contour surgery and some facial esthetics
In office
- Skin cancer care
- MOHS reconstruction
- Upper eyelid Blepharoplasty (reduction)
- Fat injections to hands, rejuvenation
- Wound Care Skin grafting and minor flaps
In the main operating room
- Complex skin cancer
- Frozen section cancer biopsy
- Tummy Tuck
- Breast reduction
- Major wound reconstruction with flaps and skin grafting
Thumb Basal Joint arthritis
Like most hand surgeons, I take the approach that we trial hand therapy and bracing for 6 weeks. If this fails you have the choice of a simple fat injection into the joint as an office procedure or a formal arthroplasty procedure in the main operating room.
Fat vs Steroid Injections
I was traditionally taught to inject the basal joint with steroids before considering surgery, but I have moved towards using autologous (your own) fat. This may be drawn off your abdomen under local anesthetic and injected into the joint, which is also first numbed. If a patient requests I will inject steroids, but it has a fixed duration of action and may attenuate your joint stability.
Autologous fat contains stem cells, and data from many studies supports that this has a beneficial effect on joint pain. In my experience since 2023 it works about 70% of the time, for an unknown duration at this time.


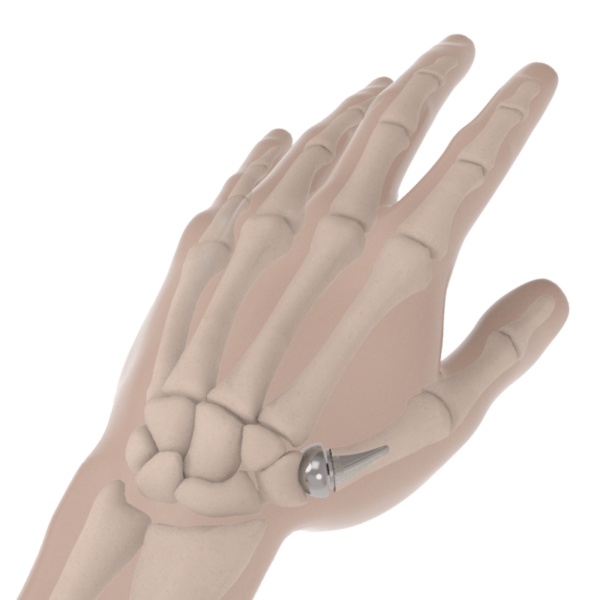
Trapeziectomy With Suspension vs Biopro Implant
- For two decades I have offered a trapeziectomy, removal of the arthritic bone under the thumb.
- I reconstruct the ligaments with an Arthrex Fibrelock bone anchor to suspend the thumb.
- Pros: Very reliable outcome with long term stability and endurance
- Cons: May reduced had grip strength 15%
I now offer younger patients with more strength requirements a Biopro implant.
- Pros: Better strength
- Cons: Implants are less stable and because you are younger it may need revision one day
Carpal tunnel syndrome
- This is caused when the tendons swell and compress the median nerve within the wrist.
- It affects over 8 Million people in the US each year.
- Previous carpal tunnel surgery over 10 ago is common
- The commonest causes include
- Diabetes
- Autoimmune diseases such as rheumatoid and lupus.
- Low Thyroid and repetitive stress may also contribute.
- Pregnancy is a very common temporary cause
- Symptoms:
- Affects the thumb index and middle finger.
- Night pain and burning.
- Pain.
- Tingling and numbness.
- Dropping objects.
- Fingers feel stiff and swollen in the morning
- Sleep deprivation causing anxiety and depression.
- Pain may radiate from hand to shoulder.
- Investigations:
- Electromyogram (EMG)
- Treatment:
- Mild to moderate disease cock-up night splints
- Moderate to severe disease: Carpal Tunnel release
- You have 2 choices for you carpal tunnel release
- Open carpal tunnel release in the office setting
- Pros: All the convenience of office surgery
- Cons: A simple incision must heal for 2 weeks
- Open carpal tunnel release in the office setting
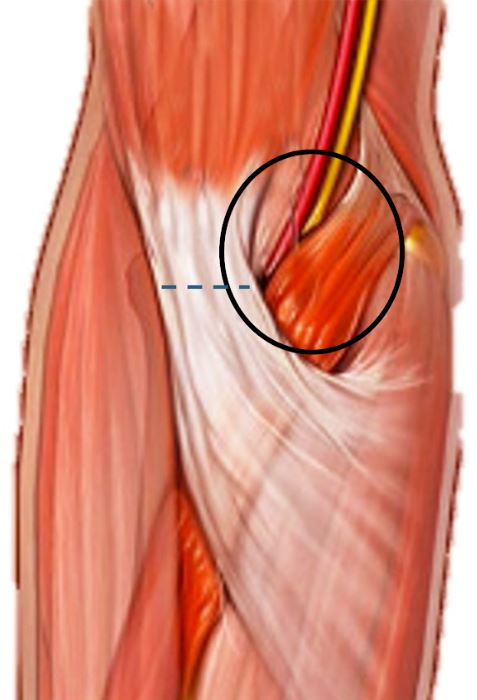
Lacertus Fibrosis Syndrome
- For many patients who have carpal tunnel syndrome-like symptoms, the median nerve can be entrapped just in front of the elbow under the “lacertus fibrosis”.
- It is not mutually exclusive from classic carpal tunnel syndrome and may coexist
- Causation:
- They may be provoked by muscular activity and is though to be due to the muscles being swollen causing the median nerve to become trapped by the non elastic tissue called the Lacertus Fibrosis
- This often only arise when a previous carpal tunnel release has failed to resolved their symptoms of tingling
- Symptoms:
- Classic numbness and tingling with burning affecting the hand
- Symptoms seem to get worse during the working day, and resolved with rest
- Symptoms commonly cause the thumb on the affected hand to become weak.
- Treatment
- Simple release of the Lacertus Fibrosis under local anesthesia.
Cubital Tunnel Syndrome
- The ulnar nerve is compressed behind the “funny bone” at the elbow
- Causation:
- Diabetes
- Previous elbow trauma
- Age related changes
- Sleeping with elbows bent
- Symptoms
- Symptoms may be subtle, particularly in older men
- Made worse with elbow flexed
- Tingling and pain and numbness to the ring and little finger
- Weakness of grip
- Clumsiness and loss of finger dexterity/ hand writing deterioration
- Later features:
- Wasting of the hand muscles
- Deformity of the little and ring finger to and “Ulnar Claw”
- Later features:
- Pathology:
- If neglected can cause the hand to become crippled with muscle wasting
- Most of the ulnar nerve serves the small muscles that coordinate our fingers, so it is not always noticed before muscle damage has occurred.
- Once “axonal nerve damage” has occurred to the nerve associated with muscle wasting, full recovery is seldom possible
- I have seen this process occur over a period of weeks.
- Investigations:
- Electromyogram (EMG)
- Treatment:
- Non operative:
- For early disease in younger people, nerve gliding occupational therapy and night elbow splints may arrest the disease
- Operative
- For most I recommend a Cubital Tunnel release in the office environment
- 2 week recovery until healed, 6 weeks 5 lb limit.
- Non operative:

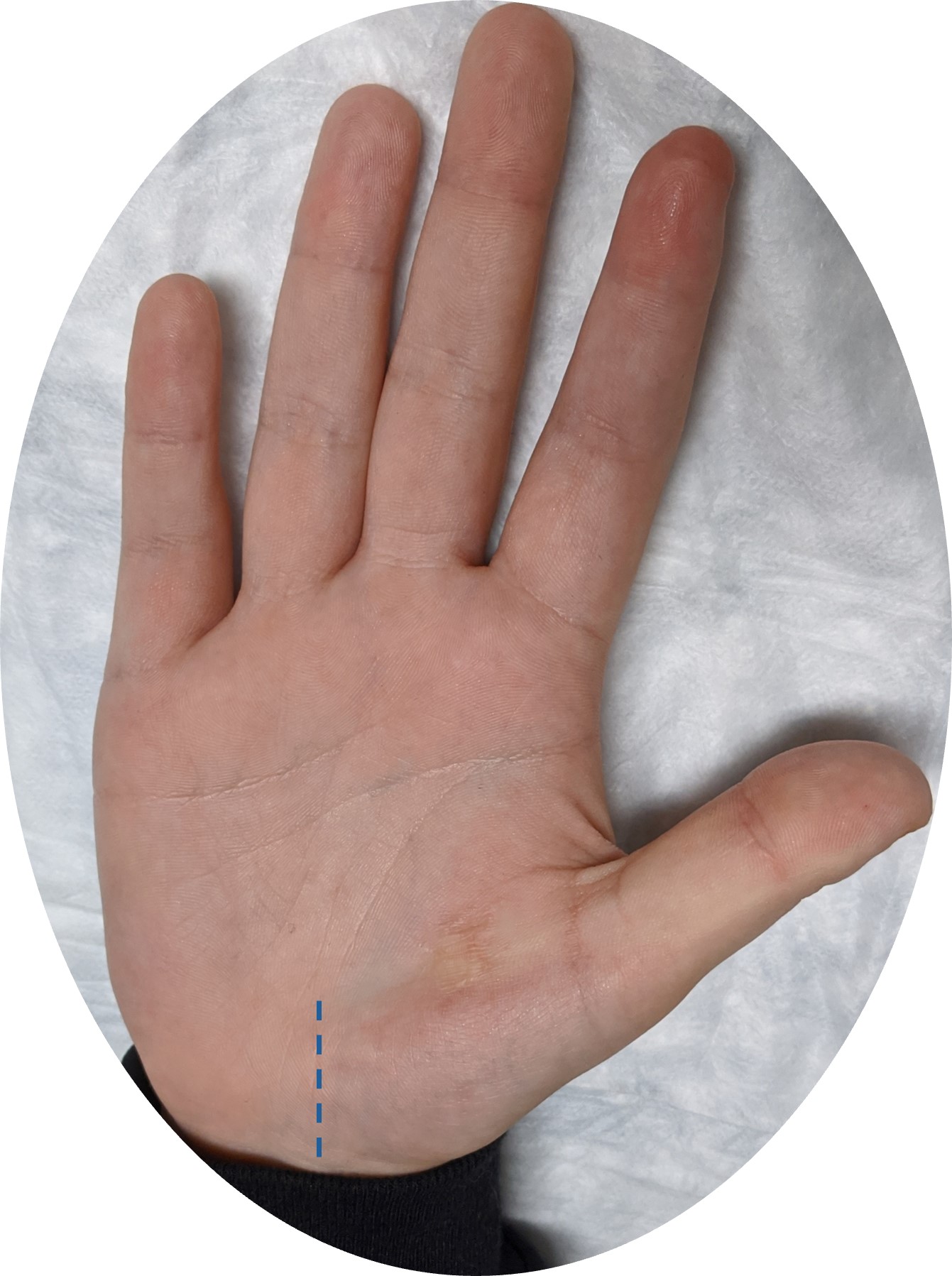
Gyon’s Canal Syndrome
- Causation:
- This a rare variant of cubital tunnel syndrome where the neve is compressed at the level of the wrist
- Very similar presentation to cubital tunnel symptoms
- This a rare variant of cubital tunnel syndrome where the neve is compressed at the level of the wrist
- Symptoms:
- Tingling and pain and numbness to the ring and little finger
- Weakness of grip
- Clumsiness and loss of hand writing
- Later wasting of hand muscles with “ulnar claw”.
- Pathology:
- If neglected can cause the hand to become crippled with muscle wasting
- Most of the ulnar nerve serves the small muscles that coordinate our fingers, so it is not always noticed before muscle damage has occurred.
- Once “axonal nerve damage” has occurred to the nerve with muscle wasting, full recovery is seldom possible
- Investigations:
- Electromyogram (EMG)
- Treatment:
- Early surgical release is important, may be performed in the office
Dupuytren’s Disease
- The genetics for this hand contracture have been traced back to our Neanderthal ancestors
- Causation:
- The body lays down scar tissue in front of the tendons of the hand
- Symptoms:
- It creates a progressive flexion deformity of the fingers, starting usually in the palm of the hand
- It affected the little and ring finger most commonly, it may affect all the palm and fingers and thumb
- “Garrod’s pads”/ Knuckle pads may also appear
- It affects more men than women and men get it at a younger age of onset
- It is gradually progressive.
- It tends to come back over time or affects other fingers
- Reasons to have surgery:
- As the fingers become contracted you will benefit from a release surgery
- Surgery may be done in the office setting
- The Dupuytren’s may simply be release with a few small incisions (Fasciotomy)
- Pros: Smallest surgery (2 week recovery, 6 weeks hand therapy)
- Cons: Does not last as long (1-3 years)
- The disease may be completely cut out (Fasciectomy), most common choice.
- Pros: Last 5-10 years before recurrence
- Cons: Longer recovery, (2-3 weeks to healing, 6 weeks hand therapy)
- The Dupuytren’s may simply be release with a few small incisions (Fasciotomy)
- When do I not advise surgery:
- When the disease is only in the palm, unfortunately surgery is not found to be helpful because it causes significant scarring for little gain.
- Is there a role for alternatives to surgery?
- Radiation therapy can help and rarely I will send a patient for a consultation to help reduce the need for surgery.
- Xiaflex is a chemical that dissolves our soft tissue, I no longer make use of this product preferring to offer surgery under local anesthesia in the office for the same advantages and less cost and risk.

Ganglion cysts
- Ganglions are very very common from childhood to old age.
- They come and they go.
- They used to be called “bible cysts”.
- They may be painful or unsightly.
- They may be found around the fingers palms and wrists.
- Cause:
- They are a leak of synovial fluid or a build up of synovial tissue from either tendons or joints.
- Treatment
- Steroid injection and aspiration works roughly 50% of the time.
- Waiting for the ganglion to burst naturally is natures way and my best advice.
- The ganglion may be excised under local anesthesia or in the main operating room under sedation.

Mucous Cysts
- This is a special form of ganglion that causes deformity of the nail plate and is hard to manage without minor surgery.
- It may leak clear jelly fluid from under the nail with a high risk of infection
- Infection may penetrate back into the joint, so never puncture your mucous cysts
- Treatment:
- The cysts must be excised back to the joint and you may require a small local skin flap to reconstruct the nailfold.

Trigger finger
- Tigger finger is an incredibly common problem and painful complaint
- Causes:
- Older age
- Diabetes
- Autoimmune diseases such as Rheumatoid and Lupus
- Low Thyroid and repetitive stress may contribute
- A previous finger sprain may set it off
- There is a very strong relation between triggering and carpal tunnel syndrome because both are caused by inflamed tendons
- What happens:
- The tendons in the fingers swell up, creating a nodule that stuck under the A1 pulley in the palm
- The finger will “catch” as you flex it
- Finger flexion is tender and painful
- The finger may painfully lock in a flexed or open position
- Treatment
- Non surgical
- 1-2 Steroid injections 6 weeks apart work 50-70% of the time
- Trigger braces
- Surgical
- Percutaneous or open trigger release
- Percutaneous release is permed under local anesthesia in office with a needle,
- Pros: It is my prfered methos, no wound, simle bandaid
- Cons: recovery may be hindedeed by inflammation in the tendon itself
- Open release is performed under local anesthesia in the office
- Pros: May be needed if recurrent/complex
- Cons: Need stitches, keep hand dry, scarring may develop.
- Non surgical
- Outcome expectations:
- Triggering may have resolved but the local tendonitis may still take months to resolved after release.
De Quervain’s Tenosynovitis/ Radial Styloiditis
- Symptoms:
- Like Trigger Finger, Dequervain’s/Radial Styloiditis is inflammation of a tendon that get trapped in a tunnel
- The tunnel in found on the side of the wrist just behind the thumb
- Pain sharply radiates from the thumb and backwards up the forearm.
- It is hard to use the thumb
- Who gets its
- Men and women of all ages
- There is a well known variant seen in mothers of babies called “Mommies Thumb”
- Causes:
- Pregnancy
- Older age
- Diabetes
- Autoimmune diseases such as Rheumatoid and Lupus
- Low Thyroid and repetitive stress may contribute
- A previous finger sprain may set it off
- Treatment
- Non surgical:
- 1-2 steroid injections 6 weeks apart get rid of about 50-70% of cases
- Thumb bracing
- Surgical:
- Open release of the tendon followed by 2 weeks of thumb bracing, this may be done in the office.
- Non surgical: